

Red Meat and Diabetes Part 1: Is it science? Is it ethical?
The crisis - 1

There is no evidence — no prior experimental observations or inherent biochemical reason — that would make you think that red meat constitutes a significant risk for type 2 diabetes. Type 2 is a disease of the glucose-insulin axis. It may play out as disruptions of lipid metabolism or other metabolic effects but there is no suggestion that red meat is a major factor. The recent publication on “Red meat intake and risk of type 2 diabetes in a prospective cohort study of United States females and males” (Gu, et al. [1]) is another epidemiological study with no clear scientific rationale and minimal associations. Contradictory evidence was not cited. The media — Forbes, The New York Times, everybody — acted as if it were the smoking gun they’ve been waiting for. It did receive some criticism. Nina Teicholz and Zoë Harcombe have provided exhaustive and very informative analysis of just how bad it was. I am adding here my own objections.
Demonstrating a significant role for red meat in diabetes would require extensive evidence but, in fact, the statistics are weak and are presented in a misleading fashion. My analysis below shows, in fact, virtually no reliable association. Most important, the paper does not address published contradictory evidence indicating an inverse relation between the consumption of red meat and the incidence of diabetes — less red meat, more diabetes. I remember. It was almost ten years ago that I presented that evidence to the authors as a letter to the editor in answer to their previous publication. Letters to the editor in the journal don’t allow figures but my figure was published by me and others over the years.
My previous letter to the editor and the reply.
To the Editor
The recent study by Pan et al [3] contains the disclaimer “Since our study is observational in nature, causality cannot be inferred.” The authors nonetheless infer that their “results add further evidence that limiting red meat consumption over time confers benefits for T2DM prevention.”
Observational studies, however, can imply causality. Bradford Hill [4] provided guidance on when associations might support causation. Hill was clear that his nine rules derive from common sense….Perhaps most telling is Hill’s principle of coherence: “data should not seriously conflict with the generally known facts of the natural history and biology of the disease.” In fact, red meat consumption decreased as T2DM increased during the past 30 years. The poor association and lack of biological plausibility suggest that the “robust” message from Pan et all is that there is no reason to associate red meat with T2DM.
Richard Feinman, PhD
In Reply
We appreciate Dr Feinman’s comments on our recent publication of changes in red meat consumption and subsequent risk of type 2 diabetes mellitus (T2DM)… “In fact, red meat consumption decreased as T2DM increased during the past 30 years.” However, this ecological relationship cannot be used to argue against the causal relationship between red meat intake and T2DM because many other factors have changed over time. (My emphasis).
An Pan, PhD
Frank B. Hu, MD, PhD
It would be good if the scientific community considered the question: if observational data do not indicate some degree of causality, should it be published? The real question, though, is that scientific practice expects authors to consider contradictory evidence: the figure above shows an association with big changes in the opposite direction.
I don’t know whether the relationship is best categorized as “ecological” but it is unlikely that nutritional epidemiology has a higher standard of reliability than ecology. Ecology is based on real measurements. Oddly, the first line of Gu, et al.: “Type 2 diabetes (T2D) is a major public health concern globally, and both the incidence and prevalence are increasing rapidly.” Data on meat consumption, however, universally indicate decreases in red meat and increases in poultry.
The data.
This was also an observational study. It was big. The “study included 216, 695 participants (81% females) from the Nurses’ Health Study (NHS), NHS II, and Health Professionals Follow-up Study (HPFS). Red meat intakes were assessed with semiquantitative food frequency questionnaires (FFQs) every 2 to 4 y since the study baselines. We used multivariable-adjusted proportional hazards models to estimate the associations between red meats and T2D. My emphasis indicates the questionable level of reliability. The authors explain that testing subjects’ perception against weighed diet records represents a methodological advance. They provide both raw data and “calibrated intake” in Table 2 (excerpt shown below). The extent of error between the raw and the calibrated data is surprising even given the food frequency method. In the Nurses Health Study, for example, intake data was off by 19 % in Q5 and 31 % in Q1. NHS and NHS II have significantly different intake. Others have pointed out the unreasonable low caloric intake and the fact that the women were out-eating the men. The paper is full of disclaimers, corrections, models and excuses. The real problem is interpretation of the data.
Understanding risk.
To report these kinds of results, different statistics can be used. I give a capsule description of some traditional ones at the end of this post (so you can recognize the terminology) but you can skip that if you like. I will just use a common sense approach to bring out the impact of the association.
First, the general sense that people often have about this kind of data is that relative statistics represents the risk of developing diabetes compared to not developing diabetes. That’s not it. The low red meat group, in fact, had 3,187 people who develop diabetes. That’s a lot. Calculations are in the next paragraph. You can skip it if you just want to see the conclusion.
The calculations in the paper are mostly corrections and confounders but what they come up with is HR (“hazard ratio”). Again, this is not giving the ratio of diabetes from red meat compared to no diabetes with no red meat. The meaning of HR is a comparison of outcomes for high red meat — roughly how much diabetes — to outcomes for low red meat (diabetes with low red meat). The data were presented as different models. Model 1, for example, “was stratified jointly by age in months and calendar time in 2-y groups and adjusted for total energy intake” although it is not indicated just how it was adjusted. For this model, the HR is 1.56, that is, about one and a half times as much diabetes in Q5 vs Q1. Describing it in terms of odds gives about 60:40. In other words, removing red meat is not a miracle cure. How much would you change your lifestyle for 60:40 odds? And that’s a model. Is it a good model? No way to tell. This kind of epidemiology is not testable. In fact, the authors continue their analysis with model 3 which has an HR of 1.21. This gives odds of 55:45. That’s too close to even odds for me. This may be an approximate value, still subject to refinement but remember, Gu, et al. are challenged to produce results that will reverse the direction of the “ecological data.” As here, statistics is often presented and used in a technical and frequently cut and dried robotic way. It’s better to just recognize what question you’re asking.
My analysis
Here’s the data from the study. Adding up all of the subjects (the top line of the figure: NHS (n = 84,31), NHS II, etc.), we get 216,695 total participants. They are broken up into five groups (quintiles, Q) according to how much red meat they consume. So each group has 216,695 / 5 = 43339 people. There is a high red meat group (Q5) and a low red meat group (Q1).
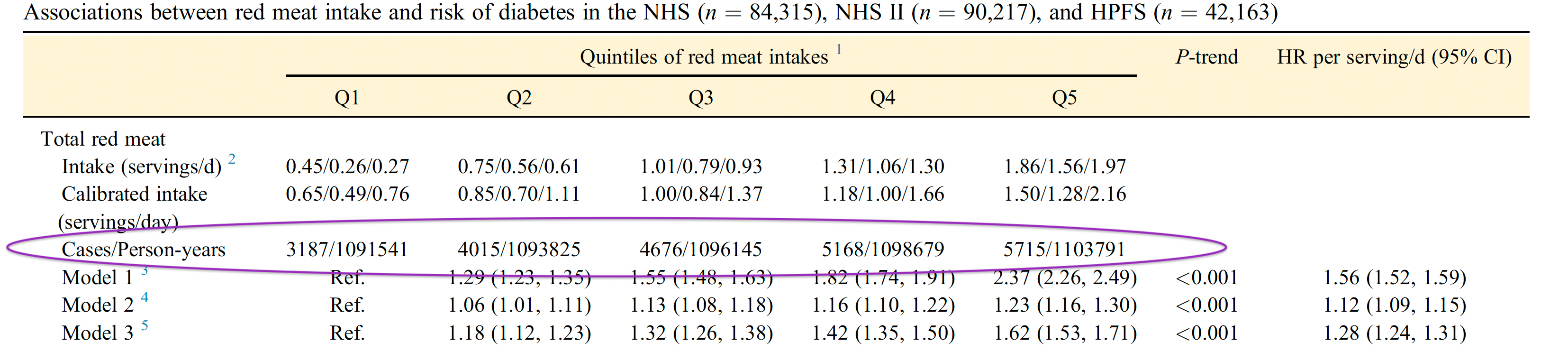
Question 1. If you are in the high red meat group, what is the probability that you will have diabetes. In other words, did the members in quintile 5 have a high incidence of diabetes and how did that compare to quintile 1, the low red meat group? The Table shows that Q5, the high meat group, had 5, 715 cases. An estimate of Risk is then = (cases in Q5) /(total number of people) = 5, 715 / 216,695 = = 0.0263 or 2.63 %. That’s a pretty low risk. But type2 diabetes is a very serious disease and, in fact, we are talking about 5,715 cases if you take the chance with high red meat. So what would we gain by reducing red meat?
The expectation is that if you go to the lowest average meat intake, Q1, you are pretty much safe. But are you? This group has 3,187 cases. That doesn’t sound so good. But, again, where does that fit into the whole population? The risk of 3187 / 216,695 = 0.0147 = 1.47 %. So, the difference in risk between high red meat and low red meat is a 2.63 - 1.47 or 1. 16 %. The difference is only slightly better than 1 in 100 that you could improve things by reducing red meat. Maybe we should look at things a different way.
Question 2. If you have diabetes, how likely is it that you are a big red meat eater? The authors describe progressive change in risk with increasing red meat. So how different are the results that would be attained if red meat had no effect — that is, if risk were independent of red meat. In that case, each quintile would have the same number of cases. The figure below reproduces the outcome data and calculates the per cent of diabetes cases for each quintile. The dotted line is the control, the calculation for Q5 as an example = (cases in Q5) /(total number of cases of diabetes) = 5,715 /22,761 = 25.1 %

Now, “HR” means hazard ratio which includes a time factor so person-years may be a rough indicator. So, we can also calculate the difference in quintiles based on person-years. I also added a dotted line in this figure that, again, tells you what the outcome would be if the risk were evenly divided into the five groups, that is, no association between red meat Q’s and the cases or the person-years. In this case, the absolute difference between high an low red meat intake is 0.2 %. Thus, using person-cases data, there is essentially zero difference in the effect of red meat.

The bottom line.
The threat of diabetes from red meat consumption proposed by this study is not real. The counter-example from the supply data has not been addressed, never mind refuted. It was a reasonable starting point for the study to have addressed the nutrient most likely to bear on origins of diabetes: carbohydrate. That data is not presented although carbohydrate consumption in the study was undoubtedly available. In fact, if you search the pdf of the paper on “carbohydrate,” you get only one hit, the title of a paper listed in the References. Is it ethical to publish data like this with such a clear recommendation? Next post in a few days.
References
Gu, X, Drouin-Chartier, J-P, Sack, FM, Frank, FB, Rosner, B. Willett, WC. Red meat intake and risk of type 2 diabetes in a prospective cohort study of United States females and males. Am. J. Clin. Nutr.. (2023) 118, 1153-1163. DOI: 10.1016/j.ajcnut.2023.08.021.
Feinman, RD, Red Meat and Type 2 Diabetes Mellitus. JAMA Internal Medicine (2014) 174, 646-647. DOI: 10.1001/jamainternmed.2013.12869.
Pan A, Sun, Bernstein AM, Manson JE, Willett WC, Hu FB. Changes in red meat consumption and subsequent risk of type 2 diabetes mellitus: three cohorts of US men and women. JAMA Intern Med. (2013) 173, 1328-1335. DOI: 10.1001/jamainternmed.2013.6633.
Hill AB. The environment and disease: association or causation? Proc R SocMed. (1965) 58, 295-300. DOI: 10.1177/0141076814562718
Add on: Short description of statistical terms.
Simplest is risk. In this context, “Risk” means probability:
The number of subjects who developed diabetes divided by total number of subjects. (By analogy with game of chance, number of ways of winning divided by all possible outcomes). You can compare two groups by calculating Relative Risk (RR) which is what it sounds like: risk (probability of winning) for one group divided by risk for the other group..
Odds tells you the number of people who developed diabetes divided by the number in the same group who didn’t. (It is the number of ways of winning divided by number of ways of losing). For comparison of two groups, you get the odds ratio (OR), obviously odds for one group divided by odds for another.
“Hazard” is slightly complicated: it is like risk (probability) but has a time component and may be more difficult to calculate. Hazard Ratio (HR) is what it sounds like.
The good news is that in cases where there is relatively small number of cases, the three measures are pretty much the same. And you can use whichever is possible to get at least a ballpark estimate of the comparisons.
Several good comments below from Eva Fain on role of glucagon. My YouTube has some basic background but still relevant. https://www.youtube.com/watch?v=STzB2USmKBg
https://ec.bioscientifica.com/view/journals/ec/aop/ec-23-0161/ec-23-0161.xml